TL;DR
- Early financial assistance screening is vital to reduce bad debt as traditional collection practices fail with higher out-of-pocket costs and deductibles increasing self-pay volume.
- Implementing a hospital presumptive eligibility program leverages self-reported data to instantly enroll eligible patients in temporary Medicaid, improving cash flow and securing immediate reimbursement.
- Front-end automation optimizes the hospital presumptive eligibility application process, it captures patient data before discharge, removes administrative burden and prevents costly third-party collection cycles.
- Integrating automated pre-screening tools allows hospitals and health systems to accurately separate charity care from bad debt, protect liquidity, and establish a clear internal payment plan.
Table of Contents
Traditional collection practices are falling short. Self-pay volume is spiking alongside high deductibles and skyrocketing out-of-pocket costs. Patients default on bills they can’t afford. This reality creates an unsustainable administrative burden for billing departments trying to establish a viable payment plan or clean up balances after care is delivered.
Intervention needs to move upstream. Provider organizations should identify qualifying patients immediately and implement a robust hospital presumptive eligibility program. This shields the revenue cycle from predictable bad debt while securing critical financial assistance for vulnerable populations.
What is Hospital Presumptive Eligibility?
Hospital presumptive eligibility empowers participating hospitals to screen patients and immediately enroll them in temporary Medicaid coverage. It was established under federal Medicaid guidelines. Decisions rely on preliminary, self-reported data like household income and family size. Hospital staff don’t have to wait for formal state verification to make the determination.
Proactive Shift to the Point of Admission
The immediate coverage window ensures the healthcare organization receives prompt reimbursement for services rendered during that period. It alters the initial patient encounter. Your financial counselors establish a pathway toward verified insurance coverage instead of categorizing an uninsured individual as a high-risk self-pay account. This proactive shift reduces uncompensated care write-offs immediately. It turns an administrative cost center into a reliable source of regulatory compliance and revenue recovery.
Optimize the Hospital Presumptive Eligibility Application Process
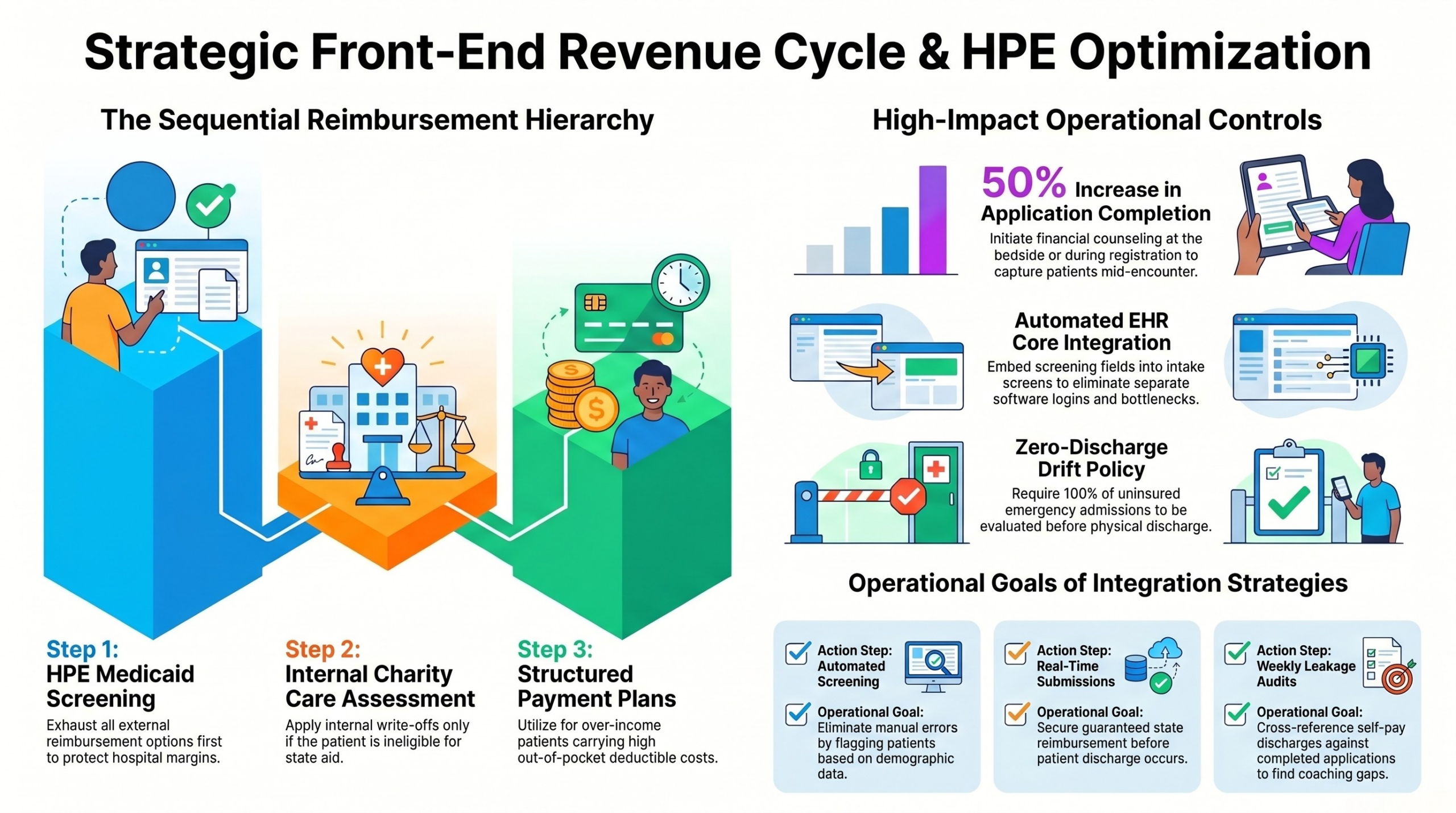
A major roadblock to programmatic success is execution at the point of entry. A streamlined hospital presumptive eligibility application process requires tight alignment between front-end clinical access points and back-end financial operations. Counselors must be positioned strategically within emergency departments and urgent admission centers. Minutes matter. Capturing patient information during the initial registration window maximizes the likelihood of submission success.
Overcome the Post-Discharge Drop-Off
Screening must occur prior to clinical discharge. Once a patient leaves the physical facility, contact conversion rates drop by over 50%, pushing the account directly toward expensive third-party collection cycles.
Automation plays an essential role here. Modern revenue cycle platforms can pre-screen admissions using credit data and geographic metrics to flag candidates before a staff member even approaches the bedside. This data-driven targeting ensures limited staff hours are focused on the highest-yield accounts. Plus, it limits friction during a highly stressful patient encounter.
Strategic Benefits for the Revenue Cycle
Transitioning patients from self-pay to temporary Medicaid yields financial improvements across the entire balance sheet.
Improving Cash Flow and Reducing Collection Costs
Waiting months for a standard Medicaid determination hurts liquidity. Presumptive approval creates an instant billing pathway. Hospitals can submit clean claims for immediate processing, radically shortening days sales outstanding (DSO) for historically problematic accounts. This faster cycle injects predictable cash flow into operations when it matters most.
Chasing self-pay balances is expensive. Staff spend hours sending statements, managing phone queues, and negotiating a low-dollar payment plan that frequently defaults anyway. When you enroll a qualified patient at the point of care, you completely eliminate downstream collection efforts. The account resolves cleanly. Staff can redirect their attention to complex commercial denials and high-value payer challenges.
Differentiating Charity Care from Bad Debt
Clear differentiation between bad debt and charity care is critical for maintaining tax-exempt status and securing local regulatory approval. Presumptive metrics allow health systems to categorize write-offs accurately. If a patient qualifies but fails to complete the full state application later, the initial window remains covered. Any subsequent non-covered balances can be routed directly into the internal financial assistance program rather than standard bad debt pipelines. This keeps collections clean.
Build a Sustainable Financial Assistance Framework
Presumptive Medicaid is a powerful tool, but it can’t solve every self-pay challenge. Patients with high deductibles often earn too much to qualify for state aid but still face bills they cannot pay out of pocket. A comprehensive revenue health strategy must pair presumptive screening with flexible internal payment options. When state aid is unavailable, clear financial assistance policies must take over seamlessly.
Transparency matters. Training front-end teams to discuss financial options openly builds trust. It changes the patient relationship from adversarial to supportive. When individuals see that a hospital is actively working to lower their financial strain, they are far more likely to engage with remaining balance obligations.
The financial health of your health system relies on moving screening processes to the front of the care timeline. Audit your current emergency department registration workflows this week. Determine what percentage of uninsured admissions leave without a formal financial screening. If your team is not utilizing presumptive tools daily, you are leaving guaranteed reimbursement on the table and driving up operational costs unnecessarily. Partner with your revenue cycle technology vendors to integrate automated pre-screening tools and protect your bottom line from avoidable self-pay losses.